
Dr. James Manos (MD)
January 5, 2016
Review: Tips in Medical Biochemistry
Volume (9)
CONTENTS
SECONDARY HYPERTENSION
Secondary hypertension
Secondary hypertension – common causes
Diagnostic algorithm for secondary hypertension
ACUTE CORONARY SYNDROME (ACS) & TROPONIN
Cardiac markers for myocardial infarction (MI)
Causes of Acute Troponin Elevation
Acute coronary syndrome – images:
Acute coronary syndrome – ECG (electrocardiogram)
An algorithm to rule out acute myocardial infarction (AMI)/ acute coronary syndrome (ACS) with high sensitivity cardiac troponin (hs-cTn)
GRACE calculator
Algorithm for NSTEMI (non-ST-elevation myocardial infarction)
SECONDARY HYPERTENSION
· Secondary hypertension: a type of hypertension with an underlying, potentially correctable cause. The prevalence of secondary hypertension and the most common etiologies vary by age group.
· About 5 – 10% of adults with hypertension have a secondary cause.
· Symptoms may suggest a secondary etiology (e.g., flushing and sweating suggestive of pheochromocytoma), examination findings (e.g., a renal bruit suggestive of renal artery stenosis), or laboratory abnormalities (e.g., hypokalemia suggestive of aldosteronism).
· Secondary hypertension also should be considered in patients with resistant hypertension, and the early or late onset of hypertension.
· In young adults, particularly women, renal artery stenosis caused by fibromuscular dysplasia is one of the most common secondary etiologies.
· Fibromuscular dysplasia can be detected by abdominal CT or MRI.
· These same imaging modalities can be used to identify atherosclerotic renal artery stenosis, a primary cause of secondary hypertension in older adults.
· In middle-aged adults, aldosteronism is the most common secondary cause of hypertension, and the recommended initial diagnostic test is an aldosterone/renin ratio.
· Up to 85% of children with hypertension have an identifiable cause, most often renal parenchymal disease. Therefore, all children with confirmed hypertension should have an evaluation for an underlying etiology that includes renal ultrasonography.
· Secondary hypertension – common causes:
· a) Children (birth to 12 years old) (70 – 85% presentence of hypertension with an underlying cause): renal parenchymal disease; coarctation of the aorta.
· b) Adolescents (12 to 18 years old) (10 – 15%): renal parenchymal disease; coarctation of the aorta.
· c) Young adults (19 to 39 years old) (5%): thyroid dysfunction (hyperthyroidism); fibromuscular dysplasia; renal parenchymal disease.
· d) Middle-aged adults (40 to 64 years old) (8 – 12%): aldosteronism, thyroid dysfunction; obstructive sleep apnoea; Cushing syndrome; pheochromocytoma.
· e) Older adults (> 65 years old) (17%): atherosclerotic renal artery stenosis; renal failure; hypothyroidism.
· Diagnostic algorithm for secondary hypertension:
{kind=link}
Acute Coronary Syndrome (ACS) & Troponin
· Cardiac markers for myocardial infarction (MI):
· Troponin I & T (Troponin elevation following cardiac cell necrosis starts within 2 – 3 hours, peaks in approximately 24 hours, and persists for 1 – 2 weeks).
· CK (creatine kinase) – MB (peak approximately in 10 – 24 hours).
· SGOT (AST) (assuming no further cardiac injury occurs, the AST level rises within 6 – 10 hours after an acute heart attack, peaks at 12 – 48 hours, and returns to normal in 3 – 4 days).
· LDH (peak approximately in 72 hours).
· Myoglobin (low specificity; peak approximately in 2 hours).
· Other cardiac markers under investigation: glucogen phosphorylase isoenzyme BB (GPBB; peak approximately in 7 hours) and ischemia-modified albumin (IMA; low specificity).
· Causes of Acute Troponin Elevation:
· I) Acute diseases:
· A) Cardiac and vascular diseases: ACS (acute coronary syndrome); tachyarrhythmias, acute congestive heart failure; aortic valve disease, hypertrophic, obstructive cardiomyopathy (HOCM) with left ventricular hypertrophy (LVH), hypertension- hypotension with arrhythmias; acute aortic dissection, Tako-tsubo cardiomyopathy, abnormalities in coronary vasomotion – including coronary vasospasm; cerebrovascular accident (ischemic stroke, intracerebral hemorrhage, subarachnoid hemorrhage); renal failure; medical ICU patients; gastrointestinal bleeding; hypotension / Shock.
· B) Respiratory diseases: acute PE (pulmonary embolism), pulmonary hypertension, ARDS (adult respiratory distress syndrome).
· C) Cardiac inflammation: endocarditis, myocarditis, pericarditis.
· D) Muscular damage.
· E) Infectious: sepsis; viral illness, parvovirus B19, myocardial involvement in bacterial endocarditis.
· F) Other acute causes of troponin increase:
· i) Kawasaki disease.
· ii) Apical ballooning syndrome.
· iii) Thrombotic thrombocytopenic purpura (TTP).
· iv) Rhabdomyolysis with cardiac injury.
· v) Birth complications in infants: extremely low birth weight; preterm delivery.
· vi) Acute complications of inherited disorders: neurofibromatosis, Duchenne muscular dystrophy; Klippel-Feil syndrome.
· vii) Environmental exposure: carbon monoxide (CO), Hydrogen sulfide (H2S), colchicine.
· II) Chronic diseases:
· a) Chronic congestive heart failure (CHF).
· b) ESRD (end–state renal disease).
· c) Cardiac infiltrative disorders: amyloidosis; sarcoidosis; hemochromatosis; scleroderma.
· d) Hypertension.
· e) Diabetes.
· f) Hypothyroidism.
· III) Iatrogenic disease:
· a) Invasive procedures:
· i) Cardiac: uncomplicated percutaneous coronary intervention (PCI); Htx (heart transplantation); transplant vasculopathy; congenital defect repair; RFCA (radiofrequency catheter ablation); pacing; implantable defibrillator firings; cardiac biopsy; cardiac surgery.
· ii) Non – cardiac: lung resection; postoperative non-cardiac surgery; ERCP.
· b) Non-invasive procedures: cardioversion; lithotripsy.
· c) Pharmacologic sources: adriamycin, 5-fluorouracil, herceptin (for breast cancer), sympathomimetic drugs (e.g., cocaine, ecstasy); chemotherapy; other medications.
· IV) Myocardial injury:
· i) Blunt chest injury; cardiac contusion.
· ii) Endurance athletes; strenuous exercise; vital exhaustion
· iii) Envenomation: snake, jellyfish, spider, centipede, scorpion.
· V) Other causes: burns (particularly when surface area >30%).
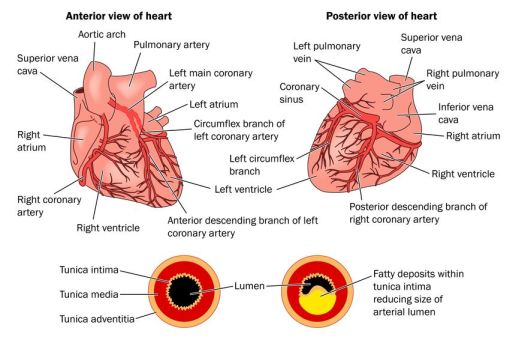
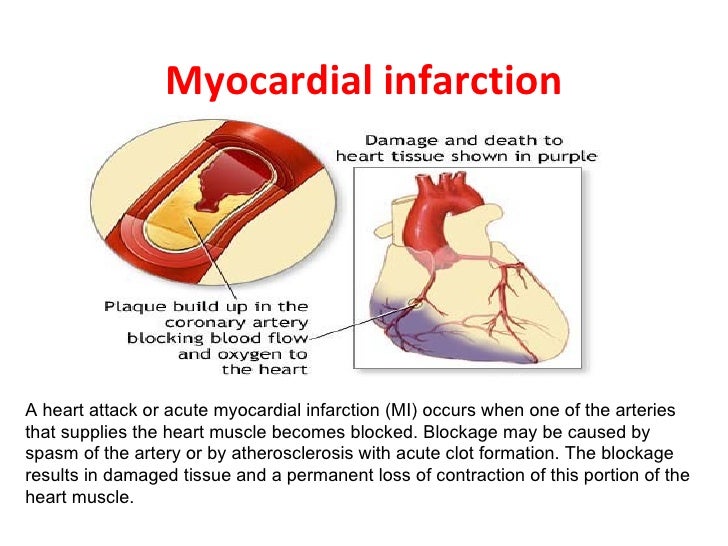
· Acute coronary syndrome – images:
{kind=link}
{kind=link}
{kind=link}
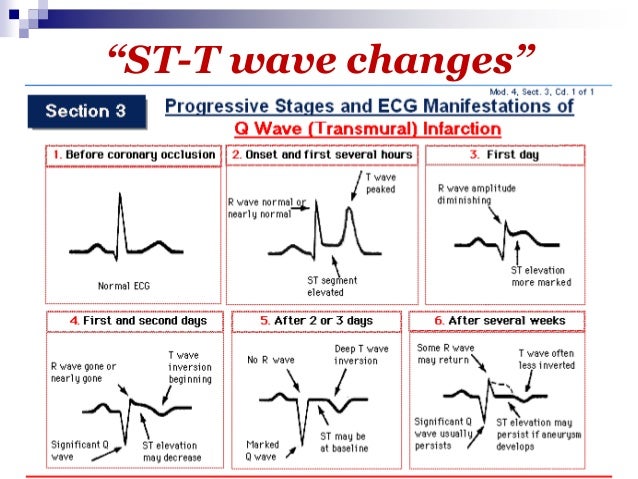
· Acute coronary syndrome – ECG (electrocardiogram):
{kind=link}
00442-9/assets/gr1.jpg){kind=link}
{kind=link}
{kind=link}
· Algorithm to rule out acute myocardial infarction (AMI)/ acute coronary syndrome (ACS) with high sensitivity cardiac troponin (hs-cTn):
{kind=link}
{kind=link}
{kind=link}
· GRACE calculator:
· Algorithm for NSTEMI (non – ST elevation myocardial infarction):
{kind=link}
{kind=link}
No comments:
Post a Comment