
Dr. James Manos (MD)
January 5, 2016
Review: Tips in Medical Biochemistry
Volume (5)
CONTENTS
ELECTROLYTE DISTURBANCES
Magnesium (Mg++)
Magnesium homeostasis
Hypomagnesemia
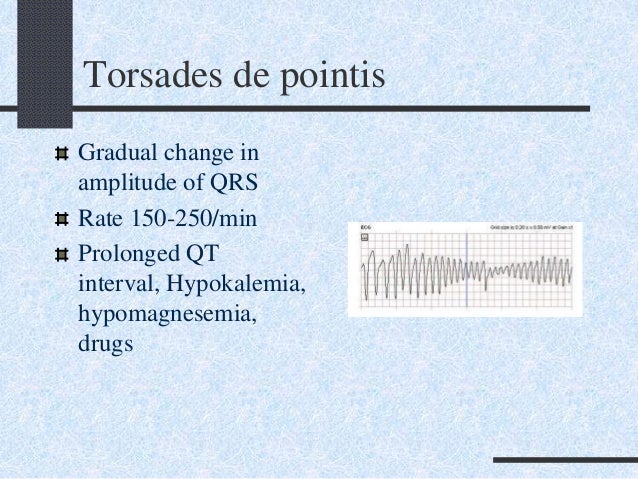
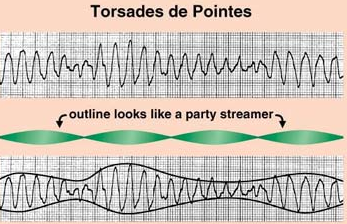
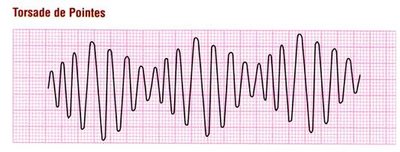
ECG (electrocardiogram): torsades de pointes
Hypomagnesemia – algorithm
Hypermagnesemia
Calcium (Ca++)
Corrected calcium
Calculator for correction of calcium on hypoalbuminemia (low blood albumin)
Ionized calcium
Calcium urine
Hypocalcemia
ECG (electrocardiogram): torsades de pointes
Causes of hypocalcemia (overview)
Laboratory evaluation of hypocalcemia
Algorithm for the evaluation of hypocalcemia
Hypercalcemia
Causes of hypercalcemia
Algorithm for the evaluation of hypercalcemia
ELECTROLYTE DISTURBANCES
· Magnesium (Mg++): it is the more prevalent intracellular cation after potassium. Normal body magnesium is about 1,000 mmol or 25 g, of which about 50% is in bone, and the other 50% is intracellular in soft tissue & muscle. Less than 1% of the total body magnesium is present in the blood. Magnesium is essential for the function of many vital enzymes, including reactions involving ATP synthesis and DNA replication, and transcription. It is also required for cellular energy metabolism, membrane stabilization, nerve conduction, calcium channel activity, and ion transport. Serum magnesium exists in three states: approximately 60% is ionized (free), 33% is protein-bound, and 7% is complex to phosphate, citrate, and other anions. About 75% of the protein-bound fraction is bound to albumin and 25% to globulins. Serum magnesium concentration does not correlate very well with tissue magnesium levels.
· Reference range: 1.4 – 2.0 mEq/L. Levels below 1.0 mEq/L are considered critical values.
· Magnesium homeostasis:
{kind=link}
· Hypomagnesemia: Hypomagnesemia is found in 12 – 20% of hospitalized patients and up to 65% of patients in intensive care units. The usual reason is the loss of magnesium from the GI (gastrointestinal) tract or the kidney. Low blood magnesium may cause ECG (electrocardiographic) abnormalities such as QT prolongation; these may degenerate to torsades de pointes; a severe arrhythmia that untreated may lead to cardiac arrest). Hypocalcemia is common in patients with severe hypomagnesemia, usually appearing when the serum magnesium level is less than 1.0 mEq/L. PTH levels are usually low and rise rapidly following magnesium replacement.
· Hypokalemia is a common event in patients with hypomagnesemia, occurring in 40-60% of cases. This is partly due to underlying disorders that cause magnesium and potassium losses, including diuretic therapy and diarrhea. It does not respond to potassium replacement until the magnesium deficit is corrected.
· Signs & symptoms: the earliest manifestations of magnesium deficiency are usually neuromuscular and neuropsychiatric disturbances, the most common being hyperexcitability. Neuromuscular irritability, including tremor, fasciculations, tetany, Chvostek and Trousseau signs, and convulsions, has been noted when hypomagnesemia has been induced in volunteers. Other manifestations include convulsions, apathy, muscle cramps and hyperreflexia.
· The classic sign of severe hypomagnesemia (< 1.2 mg/dL) is hypocalcemia. The mechanism is multifactorial.
· Parathyroid gland function is abnormal, largely because of an impaired release of PTH.
· Changes in electrocardiogram findings include prolongation of conduction and slight ST depression, although these changes are nonspecific. Patients with magnesium deficiency are particularly susceptible to digoxin-related arrhythmia. Torsade de Pointes, a repetitive, polymorphous ventricular tachycardia with prolongation of the QT interval that can lead to cardiac arrest, has been reported in conjunction with hypomagnesemia, and the American Heart Association now recommends that magnesium sulfate is added to the regimen used to manage torsade de pointes or refractory ventricular fibrillation (VF).
· It has also been suggested that magnesium plays a role in blood pressure regulation, its therapeutic efficacy in the hypertensive syndromes of pregnancy having been demonstrated.
· In epidemiologic studies, patients with CAD (coronary artery disease) have a higher incidence of magnesium deficiency than do control subjects.
· Magnesium deficiency has also been implicated in osteoporosis and kidney stones (urinary magnesium is an inhibitor of urinary crystal formation in vivo, and some studies have shown a lower urinary excretion of magnesium in patients with stones).
· Moreover, patients with diabetes mellitus are often magnesium deficient, and this decreases insulin sensitivity and secretion.
· Magnesium deficiency has also been implicated in many other conditions. Low intracellular magnesium levels in the brain have been reported in a migraine headache.
· Magnesium status may also have an influence on asthma because magnesium deficiency is associated with increased contractility of smooth muscle cells.
· The causes of magnesium depletion can be remembered as the “D” factors:
· diarrhea (lower GI secretions are rich in magnesium; diarrhea, malabsorption, bowel resection, steatorrhea, and acute pancreatitis are common causes of magnesium depletion)
· diuretics (loop diuretics can rapidly induce magnesium wasting; also long-term thiazide diuretics can cause hypomagnesemia)
· diabetes (the most common cause probably due to glycosuria and osmotic diuresis)
· drugs (especially nephrotoxic medications such as aminoglycosides, amphotericin B, cyclosporine, cisplatin, foscarnet, pentamidine)
· delivery (magnesium declines typically by 10% in pregnancy and further during labor; severe depletion is associated with pre/eclampsia)
· denuded skin (burns are associated with a general loss of electrolytes)
· dietary (hypomagnesemia becomes evident after 7 days of dietary magnesium restriction – clinical signs are observed after 42 days)
· drinking (alcohol inhibits renal tubular reabsorption of magnesium; 30% of alcoholics admitted to the hospital have low magnesium).
· Causes of hypomagnesemia – overview:
· a) Decreased magnesium intake: starvation; alcohol dependence; total parenteral nutrition.
· b) Redistribution of magnesium from extracellular to intracellular space: hungry bone syndrome (*); treatment of diabetic ketoacidosis; alcohol withdrawal syndromes; refeeding syndrome; acute pancreatitis.
· c) Gastrointestinal (GI) magnesium loss: diarrhea; vomiting and nasogastric suction; gastrointestinal fistulas and ostomies; hypomagnesemia with secondary hypocalcemia (HSH).
· d) Renal magnesium loss, including inherited renal tubular defects and drugs: Gitelman syndrome; classic Bartter syndrome (Type III Bartter syndrome); familial hypomagnesemia with hypercalciuria and nephrocalcinosis (FHHNC); autosomal-dominant hypocalcemia with hypercalciuria (ADHH); isolated dominant hypomagnesemia (IDH) with hypocalciuria; isolated recessive hypomagnesemia (IRH) with normocalcemia; HSH (hypomagnesemia with secondary hypocalcemia); diuretics (loop diuretics, osmotic diuretics, and chronic use of thiazides); antimicrobials (amphotericin B, aminoglycosides, pentamidine, capreomycin, viomycin, and foscarnet); chemotherapeutic agents (cisplatin); immunosuppressants (tacrolimus and cyclosporine), PPIs [proton-pump inhibitors such as omeprazole; they reduce gastric acid production; used e.g. on PUD (peptic ulcer disease)]; ethanol; hypercalcemia; chronic metabolic acidosis; volume expansion; primary hyperaldosteronism; recovery phase of acute tubular necrosis; post-obstructive diuresis.
· (*) Parathyroidectomy is the treatment of choice in patients with primary hyperparathyroidism (PHPT). This disease affects calcium metabolism at the level of bone tissue and renal tubules, resulting in hypercalcemia, often asymptomatic, associated with hypophosphatemia and hypomagnesemia. Sudden suppression of parathyroid hormone (PTH), caused by successful parathyroidectomy, in patients with high preoperative levels of PTH and hypercalcemia from enhanced bone turnover, may induce severe postoperative hypocalcemia that may lead to symptoms of tetany. This relatively uncommon condition is known as ‘hungry bone syndrome (HBS) because it is believed to be due mainly to an enhanced bone formation.
· ECG (electrocardiogram): torsades de pointes:
{kind=link}
{kind=link}
{kind=link}
· Hypomagnesemia – algorithm:
{kind=link}
· Hypermagnesemia is rare and usually iatrogenic. The most common causes are IV magnesium and magnesium-containing cathartics or antacids. Patients most at risk are the elderly and those with bowel disorders or renal insufficiency. Hypermagnesemia is an uncommon laboratory finding, and symptomatic hypermagnesemia is even less common. This disorder has a low incidence of occurrence because the kidney is able to eliminate excess magnesium by rapidly reducing its tubular reabsorption to almost negligible amounts.
· Signs & symptoms: Symptoms of hypermagnesemia usually are not apparent unless the serum magnesium level is greater than 2 mmol/L. Concomitant hypocalcemia, hyperkalemia or uremia exaggerate the symptoms of hypermagnesemia at any given level. Neuromuscular symptoms are the most common presenting problems. One of the earliest symptoms of hypermagnesemia is deep-tendon reflex attenuation. Facial paresthesias also may occur at moderate serum levels. Muscle weakness is a more severe manifestation that occurs at concentrations higher than 5 mmol/L. It can result in flaccid muscle paralysis and depressed respiration and can eventually progress to apnea. Hypermagnesemia depresses the conduction system of the heart and sympathetic ganglia. A moderate increase in serum magnesium can lead to a mild decrease in blood pressure, and a higher concentration may cause severe symptomatic hypotension. Magnesium is also cardiotoxic and, in high concentrations, can cause bradycardia.
· Occasionally, complete heart block and cardiac arrest may occur at levels higher than 7 mmol/L.
· Moreover, apparently, hypocalcemia results from a decrease in the secretion of parathyroid hormone (PTH) or from end-organ resistance to PTH. Paralytic ileus develops from smooth-muscle paralysis. Hypermagnesemia may also interfere with blood clotting. There has been some interest in the use of magnesium in the treatment and prevention of cardiac arrhythmias and in the treatment of subarachnoid hemorrhage; however, significant hypermagnesemia has not been reported in these settings.
· Causes of hypermagnesemia: The most common cause of hypermagnesemia is renal failure. Patients with end-stage renal disease often have mild hypermagnesemia, and the ingestion of magnesium-containing medications (e.g., antacids, cathartics) can exacerbate it. In patients with acute renal failure, hypermagnesemia usually presents during the oliguric phase; the serum magnesium level returns to normal during the polyuric phase. If a patient receives exogenous magnesium during the oliguric phase, severe hypermagnesemia can result, especially if the patient is acidotic.
· Other causes of hypermagnesemia include excessive intake; lithium therapy (causes hypermagnesemia by decreasing urinary excretion, although the mechanism for this is not completely clear); hypothyroidism; Addison disease/ adrenal insufficiency; familial hypocalciuric hypercalcemia (*), milk-alkali syndrome (**); depression; and theophylline intoxication.
· People often take magnesium-containing medications (e.g., antacids, laxatives, rectal enemas). Hypermagnesemia can develop after treatment of drug overdoses with magnesium-containing cathartics, and it also occurs in patients taking magnesium-containing medications for therapeutic purposes; however, most of these patients have a normal renal function.
· If the patient does not ingest a large amount of magnesium but has a gastrointestinal disorder (e.g., gastritis, colitis, gastric dilation), absorption may increase.
· In any case, monitoring serum magnesium levels in patients taking magnesium-containing medications is prudent.
· Excessive tissue breakdown (sepsis, shock, massive burns), especially with concurrent renal failure, can deliver a large amount of magnesium from the intracellular space, along with a massive elevation of phosphorus and potassium.
· In the treatment of eclampsia with magnesium sulfate, hypermagnesemia is induced deliberately and sometimes can be symptomatic.
· Occasionally, hypermagnesemia also can occur in the newborn infant.
· Magnesium-containing phosphorus binders are rarely used in end-stage renal disease patients and can also lead to elevated magnesium levels.
· (*) Familial hypocalciuric hypercalcemia is an autosomal dominant disorder characterized by very low excretion of calcium and magnesium and by a normal parathyroid hormone level (PTH); abnormalities of calcium and magnesium handling are due to mutations in the calcium-sensing receptor, resulting in increased magnesium reabsorption in the loop of Henle.
· (**) Milk-alkali syndrome is characterized by high blood calcium caused by taking in too much calcium and absorbable alkali; common sources of calcium and alkali are dietary supplements taken to prevent osteoporosis and antacids. If untreated, milk-alkali syndrome may lead to kidney failure.
· Calcium (Ca++): Calcium is a chemical element with the symbol Ca++ and atomic number 20. Calcium is essential for living organisms, especially in cell physiology where the movement of the calcium ion into and out of the cytoplasm functions as a signal for many cellular processes. A 70-kg person has approximately 1.2 kg of calcium in the body, more than 99% of which is stored as hydroxyapatite in bones. Less than 1% (5 – 6 g) of this calcium is located in the intracellular and extracellular compartments, with only 1.3 g located extracellularly.
· The total calcium concentration in the plasma is 4.5 – 5.1 mEq/L (9 –10.2 mg/dL). 50% of plasma calcium is ionized, 40% is bound to proteins (90% of which binds to albumin), and 10% circulates bound to anions (e.g., phosphate, carbonate, citrate, lactate, sulfate). At a plasma pH of 7.4, each gram of albumin binds 0.8 mg/dL of calcium. This bond is dependent on the carboxyl groups of albumin and is highly dependent on pH. As mentioned, approximately 99% of the body's calcium is stored in the bones and teeth. The rest of the calcium in the body has other important uses, such as some exocytosis, especially neurotransmitter release, and muscle contraction.
· In the electrical conduction system of the heart, calcium replaces sodium as the mineral that depolarizes the cell, proliferating the action potential. In cardiac muscle, sodium influx commences an action potential, but during potassium efflux, the cardiac myocyte experiences calcium influx, prolonging the action potential and creating a plateau phase of dynamic equilibrium.
· Long-term calcium deficiency can lead to rickets in children (and osteomalacia in adults) and reduced blood clotting, and in the case of a menopausal woman, it can lead to osteoporosis, in which the bone deteriorates, and there is an increased risk of fractures.
· A lifelong deficit can affect bone and tooth formation.
· However, over-retention can cause hypercalcemia (elevated levels of calcium in the blood), impaired kidney function, and decreased absorption of other minerals.
· Corrected calcium: about corrected calcium (also known as adjusted calcium) level, someone can derive it to allow for the change in total calcium due to the change in albumin-bound calcium. This gives an estimate of what the total calcium level would be if the albumin were a specified normal value. The exact formulae used to derive corrected calcium may depend on the analytical methods used for calcium and albumin. The formulas are: Corrected calcium (mg/dL) = measured total Ca (mg/dL) + 0.8 (4.0 – serum albumin [g/dL]), where 4.0 represents the average albumin level in g/dL. In other words, each 1 g/dL decrease of albumin will decrease by 0.8 mg/dL in measured serum Ca and thus 0.8 must be added to the measured Calcium to get a corrected Calcium value.
· When there is hypoalbuminemia (a lower than normal albumin), the corrected calcium level is higher than the total calcium.
· Calculator for correction of calcium on hypoalbuminemia (low blood albumin):
· IoIonized calcium: 50% of plasma calcium is ionized, 40% is bound to proteins (90% of which binds to albumin), and 10% circulates bound to anions (e.g., phosphate, carbonate, citrate, lactate, sulfate). Ionized calcium is the necessary plasma fraction for normal physiologic processes. In the neuromuscular system, ionized calcium facilitates nerve conduction, muscle contraction, and muscle relaxation.
· Ionized calcium (also called free calcium) is calcium in the blood that is not attached to proteins. For performing this lab test, the person should not eat or drink for at least 6 hours before the test. Many medicines can interfere with these blood test results. A doctor may order this test if someone has signs of kidney or parathyroid disease. The test may also be done to monitor the progress and treatment of these diseases. Most of the time, blood tests measure the total calcium level that estimates both ionized calcium and calcium attached to proteins.
· Someone may need to have a separate ionized calcium test if he/she has factors that increase or decrease total calcium levels. These may include abnormal blood levels of albumin or immunoglobulins.
· Calcium – urine: Most circulating calcium is bound to albumin. Calcium enters the extracellular fluid through absorption from the gut and resorption from bone. Calcium is cleared by secretion into the gastrointestinal and urinary tracts and also by sweating and bone deposition. The average adult has between 1 – 2 kg of total body calcium. Most of this calcium resides in the bone. Only 1% of calcium is present in the extracellular fluid.
· Causes of elevated urine calcium (the most common): hyperparathyroidism, multiple myeloma, osteolytic neoplasms, osteoporosis, vitamin D overdose, renal tubular acidosis, hyperthyroidism, Paget's disease, and sarcoidosis, drugs containing calcium (such as some antacids, and calcium supplements), spironolactone (a diuretic; it is given as calcium salt and also decreases tubular reabsorption of calcium), other medications (androgens, growth hormone (GH), acetazolamide and corticosteroids). Although not predictive of stone formation, urine calcium is frequently elevated in patients with nephrolithiasis (kidney stones).
· Causes of decreased urine calcium: hypoparathyroidism, pseudohypoparathyroidism, rickets, hypothyroidism, steatorrhea, and nephrosis, familial hypocalciuric hypercalcemia (FHH), some medications (thiazide diuretics, benzothiadiazide diuretics, and estrogen). Low-sodium diets tend to decrease calcium excretion and vice versa.
· Apparent hypocalciuria is often due to incomplete collection of a 24-hour specimen. Low-sodium diets tend to decrease calcium excretion and vice versa.
· Urine calcium levels vary with dietary intake.
· A 24-hour urine sample collected from an average healthy adult contains between 100 – 250 mg of calcium (15–20 mmol). Individuals adhering to a low calcium diet excrete between 50 and 150 mg/ day, while individuals following a strict calcium-free diet can have urine concentrations as low as 5 – 40 mg/ day. Measurement of urine calcium is used in the differential diagnosis of patients with abnormal plasma calcium levels. Urine calcium concentration can be measured in a 24-hour urine collection or a random urine sample (spot).
· Random urine calcium concentration is best expressed as the calcium to creatinine ratio (CCCR), also known as the fractional excretion of calcium. The CCCR can be calculated from simultaneous determinations of plasma calcium and creatinine along with the 24-hour renal excretions of calcium and creatinine and apply the following formula: (24-hour U-calcium/P-total calcium) / (24-hour U-creatinine/P-creatinine) = 24 - hour Urinary Calcium x Plasma Creatinine/ plasma Calcium x 24-hour Urinary Creatinine. A fasting urine sample may also be useful in diagnosing calcium overdose from antacids or supplements. If a 2-hour urine collection is obtained after a 14-hour fast, the urine calcium: creatinine ratio (CCCR) should be less than 0.15. If it is >0.15, metabolic/nephrogenic hypercalciuria is suspected.
· The reference range for calcium in a 24-hour urine collection is < 350 mg per day. A normal reference interval for the urine calcium (mg/dL) to urine creatinine (mg/dL) ratio (CCCR) is < 0.14. Values > 0.20 are found in patients with hypercalciuria. In children, the calcium/creatinine ratio decreases steadily until approximately age 6. A calcium creatinine clearance ratio (CCCR) of less than 0.010 is consistent with familial hypocalciuric hypercalcemia (FHH), whereas a CCCR greater than 0.020 is highly suspicious of hyperparathyroidism. One study revealed that a CCCR cutoff of 0.020 captured 98% of patients with FHH but also included 35% of patients with primary hyperparathyroidism. CCCR might be useful as an initial screening test for FHH, followed by CASR gene analysis for patients with a CCCR of less than 0.020.
· If adult reference ranges are used for younger children their results will be falsely flagged as hypercalciuric. Elevated urine calcium is defined as a concentration higher than 350 mg/ 24 hours.
· Hypocalcaemia is the presence of low serum calcium levels in the blood. Physiologically, blood calcium is tightly regulated within a narrow range for proper cellular processes. Calcium in the blood exists in three primary states: bound to proteins (mainly albumin), bound to anions such as phosphate and citrate, and as free (unbound) ionized calcium. Only the ionized calcium is physiologically active. Normal blood calcium level is between 8.5 – 10.5 mg/dL (2.12 – 2.62 mmol/L) and that of ionized calcium is 4.65 – 5.25 mg/dL (1.16 – 1.31 mmol/L).
· Symptoms of hypocalcemia include neuromuscular irritability (including tetany, manifested with positive Chvostek’s sign or Trousseau’s signs; carpopedal spasm and generalized tetany is characterized by unrelieved and forceful contractions of the hands and in the large muscles of the rest of the body), oral, perioral and acral paresthesias (tingling or 'pins and needles' sensation in and around the mouth and lips, and in the extremities of the hands and feet; this is often the earliest symptom of hypocalcemia), laryngospasm (characterized by stridor), electrocardiographic changes such as QT prolongation that puts the patient for risk of a severe arrhythmia (that untreated may lead to cardiac arrest) called torsades de points; petechiae, hyperactive tendon reflexes, and seizures.
· ECG (electrocardiogram): torsades de pointes:
· Causes of hypocalcemia (overview):
· a) Hypoalbuminemia. It is the most common cause of hypocalcemia. Causes include cirrhosis, nephrosis, malnutrition, burns, chronic illness, and sepsis. In patients who are critically ill, low calcium levels can be simply due to hypoalbuminemia, which has no clinical significance because the active fraction (ionized) is not affected. However, to prevent missing a second hypocalcemic disorder, ionized calcium level whenever the albumin level is low should be measured.
· b) Hypomagnesemia. Severe hypomagnesemia can lead to hypocalcemia that is resistant to the administration of calcium and vitamin D. The usual cause of hypomagnesemia is loss via the kidneys (eg, osmotic diuresis, drugs) or the gastrointestinal tract (eg, chronic diarrhea, severe pancreatitis, bypass, or resection of the small bowel). These patients present with low or inappropriately normal PTH levels in the presence of hypocalcemia.
· c) Hyperphosphatemia. It may be seen in critical illnesses and in patients who have ingested phosphate-containing enemas. Phosphate binds calcium avidly, causing acute hypocalcemia. Acute hypocalcemia secondary to hyperphosphatemia may also result from renal failure or excess tissue breakdown because of rhabdomyolysis or tumor lysis. In acute hyperphosphatemia, calcium is deposited mostly in the bone but also in the extraskeletal tissue. In contrast, in chronic hyperphosphatemia (that occurs nearly always from chronic renal failure) calcium efflux from the bone is inhibited and the calcium absorption is low, because of reduced renal synthesis of 1,25-dihydroxy vitamin D. However, other consequences of renal failure, including a primary impairment in calcitriol (1,25-dihydroxy vitamin D3) synthesis, also contribute to hypocalcemia.
· d) Multifactorial enhanced protein binding & anion chelation. Protein binding is enhanced by elevated pH and free fatty acid release in high catecholamine states. Anion chelation is seen in high phosphate states (eg, renal failure, rhabdomyolysis, mesenteric ischemia, oral administration of phosphate-containing enemas); high citrate states (eg, massive blood transfusion, radiocontrast dyes); and high bicarbonate, lactate, and oxalate levels.
· e) Surgical effect. The following surgical procedures may result in hypocalcemia:
· 1) Parathyroid adenoma resection (it causes transient hypocalcemia due to end-organ PTH resistance in the first postoperative day).
· In addition, vascular/parathyroid injury may occur as an operative mishap (unlucky accident)) such as on thyroidectomy.
· 2) Pancreatectomy (it prevents calcium absorption in the duodenum and the jejunum by eliminating necessary enzymes).
· 3) Bowel resection (it may cause hypocalcemia by reducing the surface available to absorb fatty acids and calcium).
· f) PTH deficiency or resistance/ hypoparathyroidism. Hypoparathyroidism can be hereditary or acquired.
· Acquired hypoparathyroidism may result from the following: neck irradiation/radioiodine therapy; post (after) parathyroidectomy in dialysis patients; inadvertent surgical removal (can be transient or permanent); infiltrative disease [e.g., hemochromatosis, granulomatous disease (sarcoidosis), thalassemia, amyloidosis, or metastatic malignant infiltration].
· Late-onset hypoparathyroidism can be seen as a part of complex autoimmune disorders involving ovarian failure and adrenal failure. Mucocutaneous candidiasis, alopecia, vitiligo, and pernicious anemia are associated with this disorder, which is referred to as polyglandular autoimmune disease (PGA I).
· Hereditary hypoparathyroidism may be familial or sporadic, and it can occur as an isolated entity or can be associated with other endocrine manifestations. The familial forms include autosomal dominant and autosomal recessive, as well as a sex-linked form of early-onset. Sporadic, late-onset hypoparathyroidism is a feature of several hereditary syndromes such as DiGeorge syndrome; Kearns-Sayre syndrome; and Kenny-Caffey syndrome.
· Pseudohypoparathyroidism is characterized by end-organ resistance to the effects of PTH. PTH binds to the PTH receptor, which, in turn, activates cAMP through guanine nucleotide regulatory proteins (Gs). These proteins consist of alpha, beta, and gamma subunits. It is classified into types I and II. Type I is further subdivided into Ia, Ib, and Ic.
· g) Vitamin D deficiency or resistance. Vitamin D is a necessary cofactor for the normal response to PTH, and vitamin D deficiency renders PTH ineffective. Poor nutritional intake, chronic renal insufficiency, or reduced exposure to sunlight may cause vitamin D deficiency. Numerous conditions can impair the absorption of vitamin D. Small bowel diseases, such as celiac disease, gastric bypass (particularly long limb Roux-en-Y gastric bypass), steatorrhea, and pancreatic diseases can all lead to low vitamin D levels.
· Pseudovitamin D deficiency rickets is a condition is secondary to an autosomal mutation of the 1-hydroxylase gene. Ultimately, calcidiol is not hydroxylated to calcitriol, and calcium is not absorbed appropriately. This condition is considered a pseudovitamin D deficiency because high doses of vitamin D can overcome the clinical and biochemical findings of this disease.
· Hereditary vitamin D resistance rickets is an extremely rare condition caused by a mutation in the vitamin D receptor. Typically, it presents within the first 2 years of life.
· h) Liver disease. Liver disease with decreased synthetic function can cause vitamin D deficiency from several sources: impaired 25-hydroxylation of vitamin D; decreased bile salts with malabsorption of vitamin D; decreased synthesis of vitamin D–binding protein; other factors. Patients with cirrhosis and osteomalacia have low or normal levels of calcitriol.
· i) Chronic kidney disease. Chronic kidney disease leads to a decrease in the conversion of 25-hydroxyvitamin D to its active form 1,25-dihydroxy vitamin D, particularly when the glomerular filtration rate (GFR) falls below 30 mL/min. This results in an increase in PTH. Ultimately, the increased absorption of phosphorus and calcium can lead to calcium-phosphorus mineral deposition in the soft tissues. In the early stages of renal failure, hypocalcemia can occur because of the decrease in calcitriol production and a subsequent decrease in the intestinal absorption of calcium.
· j) Pancreatitis. It can be associated with tetany and hypocalcemia. It is caused primarily by the precipitation of calcium soaps in the abdominal cavity; also glucagon-stimulated calcitonin release and decreased PTH secretion may play a role. When the pancreas is damaged, free fatty acids are generated by the action of pancreatic lipase. Insoluble calcium salts are present in the pancreas, and the free fatty acids avidly chelate the salts, resulting in calcium deposition in the retroperitoneum. In addition, hypoalbuminemia may be a part of the clinical picture, resulting in a reduction in total serum calcium.
· k) Hypocalcemic emergencies in the emergency department (ED): rhabdomyolysis [increased phosphates from creatine phosphokinase (CPK) and other anions (ie, lactate, bicarbonate) chelate calcium]; toxic shock syndrome; high calcitonin levels; malignancy [osteoblastic metastases (eg, breast cancer, prostate cancer) and tumor lysis syndrome may cause hypocalcemia by differing mechanisms]; infiltrative diseases (sarcoidosis, tuberculosis, and hemochromatosis may infiltrate the parathyroids, causing dysfunction); toxicologic causes (e.g. hydrofluoric acid burn or ingestion); and trauma patients with massive transfusion (will have hemostasis impairment as one effect of hypocalcemia due to the complex of citrate, used as an anticoagulant on blood bags, with serum calcium).
· l) Acute illness (it may lead to hypocalcemia for multiple reasons). In one study, the 3 most common factors identified in patients with hypocalcemia associated with acute illness were hypomagnesemia, acute renal failure, and transfusions. Also, in gram-negative sepsis, there is a reduction in total and ionized serum calcium.
· m) Medications:
· i) Cinacalcet (a drug indicated for the treatment of secondary hyperparathyroidism in people with chronic kidney disease on dialysis and hypercalcemia in people with parathyroid carcinoma): patients receiving the calcimimetic agent cinacalcet to help control secondary hyperparathyroidism in renal failure may experience hypocalcemia as a result of acute inhibition of PTH release; clinically significant hypocalcemia occurs in approximately 5% of patients treated with cinacalcet.
· ii) Some chemotherapeutic drugs (e.g., cisplatin can induce hypocalcemia by causing hypomagnesemia, and combination therapy with 5-fluorouracil and leucovorin can cause mild hypocalcemia in 65% of patients in one series).
· iii) On the treatment of hypercalcemia with bisphosphonates.
· iv) Prolonged therapy with anticonvulsants (eg, phenytoin, and phenobarbital; the mechanisms differ according to the class of anticonvulsants; for example, phenytoin induces cytochrome P450 enzymes and enhances vitamin D catabolism).
· v) Foscarnet (a medication used to treat refractory cytomegalovirus and herpes infections in patients who are immunocompromised; it complexes ionized calcium and, therefore, lowers ionized calcium concentrations, potentially causing symptomatic hypocalcemia).
· vi) Denosumab (a fully human monoclonal antibody to the receptor activator of nuclear factor kappaB ligand (RANKL), an osteoclast differentiating factor; it is used on osteoporosis treatment). In the denosumab trials, a small proportion of women in denosumab trials had a decrease in the serum calcium level to less than 8.5 mg/dL. However, in patients with conditions that predispose to hypocalcemia, such as chronic kidney disease, malabsorption syndromes, or hypoparathyroidism, symptomatic hypocalcemia may occur. The nadir in serum calcium occurs approximately 10 days after administration. Thus, denosumab should not be given to patients with preexisting hypocalcemia until it is corrected. In addition, patients with conditions predisposing to hypocalcemia (ie, chronic kidney disease and creatinine clearance < 30 mL/min) should be monitored for hypocalcemia.
· vii) Transfusion of citrated blood or plasma (symptomatic hypocalcemia is rare, because healthy patients rapidly metabolize citrate in the liver and kidney, however, a clinically important fall in serum ionized calcium concentration can occur if citrate metabolism is impaired due to hepatic or renal failure or if large quantities of citrate are given rapidly, for example, during plasma exchange or massive blood transfusion, due to the complex of citrate, used as an anticoagulant on blood bags, with serum calcium).
· viii) Sodium phosphate preparations (used to cleanse the bowel prior to GI procedures such as colonoscopy; in certain populations, these agents can lead to acute hyperphosphatemia and subsequent hypocalcemia).
· ix) Some radiographic contrast dyes (they may contain EDTA which chelates calcium in serum, thereby reducing serum ionized calcium concentration, resulting in hypocalcemia). Gadolinium-based contrast material can falsely lower serum calcium levels and should be considered if levels are drawn shortly after magnetic resonance imaging (MRI).
· x) Fluoride. Rarely, an excess intake of fluoride can cause hypocalcemia; this effect is presumably mediated by inhibition of bone resorption. Overfluorinated public water supplies and ingestion of fluoride-containing cleaning agents have been associated with low serum calcium levels.
· xi) Proton pump inhibitors (PPIs; e.g., omeprazole) and histamine-2 receptor blockers (e.g., cimetidine) (medications that reduce gastric acid production – used, e.g., for peptic ulcer disease and for gastroesophageal reflux disease). The reduced acid production by these drugs slows fat breakdown, which is necessary to complex calcium for gut absorption; decreased calcium absorption has been associated with increased risk for hip fractures in elderly patients.
· xii) Other medications: calcitonin & bisphosphonates (for osteoporosis; they cause chelation and end-organ inhibition); ethylene glycol (complexes with calcium); estrogen (inhibits bone resorption); and aluminum & alcohol (suppress PTH)
.
.
· Laboratory evaluation of hypocalcemia:
· Condition:
· i) Hypoparathyroidism: low PTH (parathyroid hormone); elevated phosphorus; normal 25 hydroxy-vitamin D; normal or low 1,25 dihydroxy vitamin D3.
· ii) Calcium-sensing receptor activating mutation: normal or low PTH (parathyroid hormone); elevated phosphorus; normal 25 hydroxy-vitamin D; normal 1,25 dihydroxy vitamin D3.
· iii) Pseudohypoparathyroidism (parathyroid hormone (PTH) resistance): elevated PTH (parathyroid hormone); elevated phosphorus; normal 25 hydroxy-vitamin D; 1,25 dihydroxy vitamin D3.
· iv) Vitamin D deficiency: raised PTH (parathyroid hormone); low or normal phosphorus; low 25 hydroxy-vitamin D; normal or elevated 1,25 dihydroxy vitamin D3.
· v) Chronic kidney disease: elevated PTH (parathyroid hormone); high phosphorus; normal 25 hydroxy-vitamin D; low 1,25 dihydroxy vitamin D3.
· Note: calcitriol or 1,25-dihydroxycholecalciferol or 1,25-dihydroxy vitamin D3, is the hormonally active metabolite of vitamin D. Cholecalciferol (cholecalciferol, vitamin D3) is one of the five forms of vitamin D. 7 – Dehydrocholesterol (provitamin D3) is the precursor of cholecalciferol. Within the epidermal layer of skin, it undergoes an electrocyclic reaction as a result of UVB radiation, resulting in the opening of the vitamin precursor B-ring through a conrotatory pathway. Following this, it finally isomerizes to form cholecalciferol (vitamin D3). Cholecalciferol is then hydroxylated in the liver to become calcifediol (25-hydroxyvitamin D3; also known as calcidiol, 25-hydroxycholecalciferol; abbreviated 25(OH)D). Calcifediol is then hydroxylated in the kidney, under the regulation of parathyroid hormone (PTH), and becomes calcitriol (1,25-dihydroxy vitamin D3) or active vitamin D3. See also http://www.wikipathways.org/index.php/Pathway:WP1531
· Algorithm for the evaluation of hypocalcemia:
{kind=link}
· Hypercalcaemia: Hypercalcemia can result when too much calcium enters the extracellular fluid or when there is insufficient calcium excretion from the kidneys.
· Approximately 90% of cases of hypercalcemia are caused by malignancy or hyperparathyroidism.
· Classification: Hypercalcemia may be classified based on total serum and ionized calcium levels, as follows:
· a) Mild: Total Ca 10.5-11.9 mg/dL (2.5-3 mmol/L) or Ionized Ca 5.6-8 mg/dL (1.4-2 mmol/L).
· b) Moderate: Total Ca 12-13.9 mg/dL (3-3.5 mmol/L) or Ionized Ca 5.6-8 mg/dL (2-2.5 mmol/L).
· c) Hypercalcemic crisis: Total Ca 14-16 mg/dL (3.5-4 mmol/L) or Ionized Ca 10-12 mg/dL (2.5-3 mmol/L).
· Mild prolonged hypercalcemia may produce mild or no symptoms, or recurring problems such as kidney stones. Sudden-onset and severe hypercalcemia may cause dramatic symptoms, usually including confusion and lethargy, possibly leading quickly to death. Central nervous system effects include lethargy, weakness, confusion, and coma. Renal effects include polyuria, nocturia, dehydration, renal stones, and renal failure.
· Gastrointestinal effects include constipation, nausea, anorexia, pancreatitis, and gastric ulcer.
· Cardiac effects include syncope from arrhythmia.
· A helpful mnemonic, "painful bones, renal stones, abdominal groans, and psychic moans," can be used to recall the typical symptoms of hypercalcemia.
· Causes of hypercalcemia: About 90% of cases of hypercalcemia are caused by malignancy or hyperparathyroidism. About 20 – 30% of patients with cancer have hypercalcemia during the disease, and its detection may signify an unfavorable prognosis. Of the cases due to malignancy, approximately 80% are due to bony metastases, while the other 20% are due to the effects of parathyroid hormone-related peptide (PTHrP).
· Hypercalcemia secondary to malignancy may be classified into the following four types:
· a) Humoral hypercalcemia of malignancy (HHCM) from increased secretion of PTHrP. The most common form; it accounts for up to 80% of cases.
· b) Osteolytic hypercalcemia from the osteoclastic activity and bone resorption surrounding the tumor tissue. The second most common mechanism; accounts for about 20% of cases.
· c) Secretion of active vitamin D by some lymphomas.
· d) Ectopic parathyroid hormone (PTH) secretion (very rare).
· The remaining 10% of cases of hypercalcemia are caused by many different conditions, including vitamin D–related problems, disorders associated with rapid bone turnover, thiazides (diuretics) or renal failure, and in rare cases, familial disorders. Treatment with recombinant human PTH for postmenopausal osteoporosis is also a cause.
· Overview of the causes:
· i) Causes of hypercalcemia that are related to malignancy (lung, breast, and multiple myeloma are the most common tumors) include:
· a) Solid tumor metastases.
· b) Solid tumors (especially lung, head, and neck squamous cancers, renal cell tumors) with humoral effects.
· c) Hematologic malignancies.
· ii) Causes of hypercalcemia that are related to the parathyroid:
· a) Primary hyperparathyroidism: solitary adenoma; generalized hyperplasia; multiple endocrine neoplasia (MEN) type 1 or type 2A.
· b) Tertiary hyperparathyroidism (associated with chronic renal failure or vitamin D deficiency).
· c) Lithium-related release of PTH (lithium is taken for bipolar disorder).
· d) Familial cases of high PTH levels./// Familial isolated hyperparathyroidism; Familial hypocalciuric hypercalcemia/ familial benign hypercalcemia.
· e) Neonatal severe hyperparathyroidism.
· iii) Causes related to vitamin D:
· a) Vitamin D toxicity (e.g., over–the–counter supplements).
· b) Granulomatous disease (especially sarcoidosis; also berylliosis, tuberculosis, etc.).
· c) Hodgkin’s lymphoma.
· d) Idiopathic hypercalcemia of infancy.
· e) Rebound hypercalcemia after rhabdomyolysis.
· iv) Causes related to high bone turnover:
· a) Hyperthyroidism.
· b) Prolonged Immobilization (especially in Paget disease).
· c) Thiazide diuretic use.
· d) Vitamin A intoxication.
· e) Renal failure related: milk-alkali syndrome (*); severe secondary hyperparathyroidism; aluminum poisoning.
· f) Multiple myeloma.
· v) Other causes related to particular mechanisms are: increased intestinal calcium absorption; idiopathic infantile hypercalcemia (Williams syndrome); granulomatous disorders (eg, sarcoidosis; also berylliosis, tuberculosis, etc); decreased renal calcium excretion; familial hypocalciuric hypercalcemia; increased bone resorption; mutations of the calcium-sensing receptor; familial benign hypocalciuric hypercalcemia; hypophosphatasia; subcutaneous fat necrosis; blue diaper syndrome (**); and dietary phosphate deficiency.
· (*) Milk-alkali syndrome is characterized by high blood calcium caused by taking in too much calcium and absorbable alkali; common sources of calcium and alkali are dietary supplements taken to prevent osteoporosis and antacids. If untreated, milk-alkali syndrome may lead to kidney failure.
· (**) Blue diaper syndrome is a rare, autosomal recessive metabolic disorder characterized in infants by bluish urine-stained diapers. It is caused by a defect in tryptophan (an essential amino acid) absorption. Bacterial degradation of tryptophan in the intestine leads to excessive indole production and thus to indicanuria which, on oxidation to indigo blue, causes a peculiar bluish discoloration of the diaper. Symptoms typically include digestive disturbances, fever, and visual problems.
· Algorithm for the evaluation of hypercalcemia:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
No comments:
Post a Comment